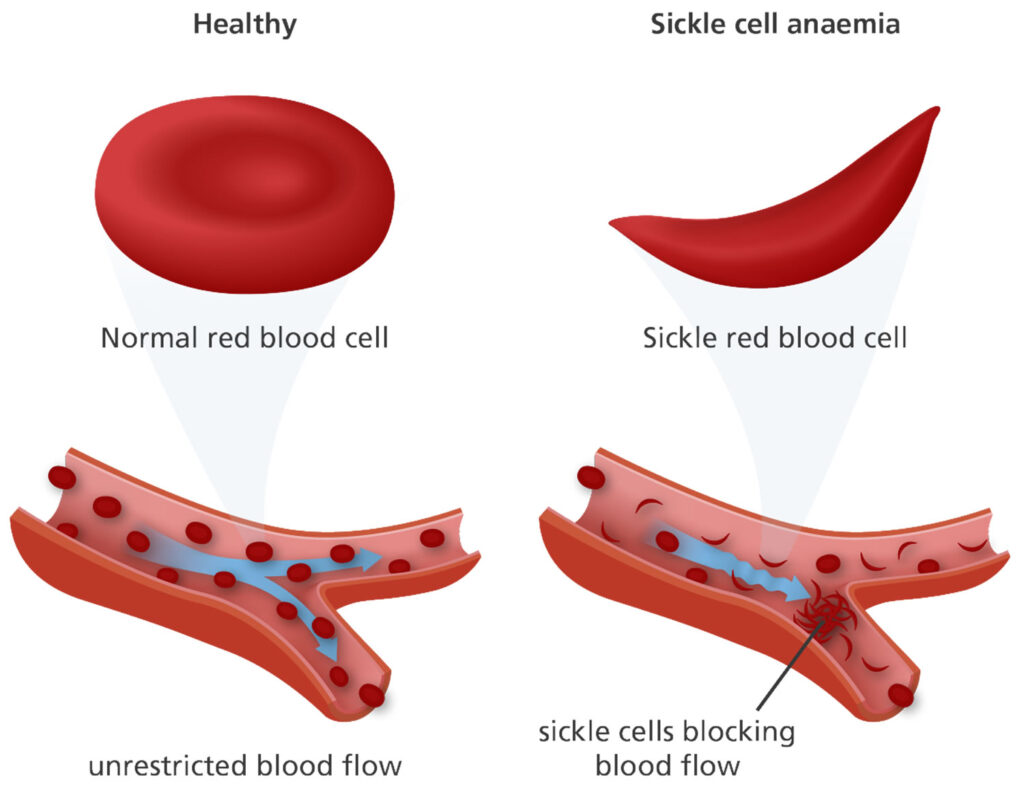
Sickle cell disease (SCD) stands as one of the most prevalent hereditary blood disorders worldwide, affecting millions of individuals, particularly those of African descent. This genetic condition alters the structure of hemoglobin, the protein responsible for carrying oxygen in red blood cells. The result is the formation of rigid, sickle-shaped red blood cells, which can obstruct blood flow, leading to a plethora of complications.
Navigating life with SCD presents numerous challenges, including acute pain crises, anemia, organ damage, and heightened susceptibility to infections. Amidst these challenges, clotting control emerges as a critical aspect of care. Effective management of clotting issues is essential to mitigate the risk of thrombotic events while addressing bleeding complications that may arise due to the unique pathophysiology of SCD.
UNDERSTANDING SICKLE CELL DISEASE
SCD is a complex genetic disorder characterized by mutations in the HBB gene, which encodes the beta-globin subunit of hemoglobin. These mutations lead to the production of abnormal hemoglobin molecules, namely hemoglobin S (HbS). When deoxygenated, HbS molecules polymerize, causing red blood cells to assume a sickle shape. This alteration in cell morphology underlies many of the clinical manifestations associated with SCD.
COMPLICATIONS ASSOCIATED WITH SCD
The consequences of SCD are multifaceted and can significantly impact the health and well-being of individuals living with the condition. Pain crises, often excruciating and unpredictable, occur due to vaso-occlusive events, wherein sickled red blood cells obstruct blood flow to various tissues and organs.
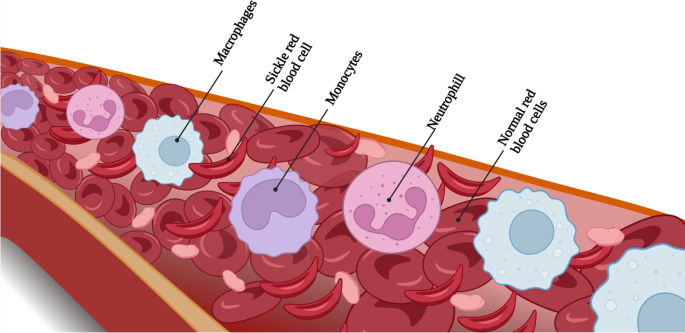
Chronic anemia results from the shortened lifespan of sickle cells, leading to fatigue, pallor, and reduced oxygen delivery to tissues. Organ damage, particularly affecting the spleen, kidneys, lungs, and brain, may occur due to repeated ischemic insults. Furthermore, the compromised immune function associated with SCD increases the risk of severe infections, posing additional challenges to disease management.
CLOTTING CONTROL IN SCD
Maintaining a delicate balance between coagulation and anticoagulation is crucial for individuals with SCD. While they are predisposed to both thrombotic and hemorrhagic complications, the underlying mechanisms driving these opposing phenomena remain incompletely understood. Abnormalities in coagulation factors, platelet function, endothelial dysfunction, and inflammation contribute to the complex interplay between clotting and bleeding in SCD.
CHALLENGES IN CLOTTING CONTROL FOR SCD PATIENTS
Managing clotting issues in SCD patients is inherently challenging due to the unique hemostatic profile of the disease. Coagulation abnormalities, including increased levels of procoagulant factors and platelet activation, predispose individuals to thrombotic events. Paradoxically, SCD is also associated with a bleeding diathesis, characterized by impaired platelet function, endothelial damage, and decreased levels of anticoagulant proteins. This duality presents clinicians with the daunting task of preventing thrombosis while minimizing the risk of hemorrhage, often requiring individualized treatment strategies.

ROLE OF PT/INR TESTING
Prothrombin Time (PT) and International Normalized Ratio (INR) testing have emerged as valuable tools in the management of clotting issues in SCD patients. PT measures the time it takes for blood to clot after the addition of tissue factor, while INR standardizes PT results across different laboratories, enabling comparability between patients.
YOU MAY READ OUR OTHER BLOGS TOO:
STROKE RISK FACTORS AND PT/INR MONITORING: A COMPREHENSIVE APPROACH TO PREVENTION
BALANCING ACT: NUTRITIONAL SUPPORT FOR ANTICOAGULATION PATIENTS
EMPOWERING HEALTH: UNDERSTANDING GENETIC PREDISPOSITION TO CLOTTING THROUGH PT/INR SELF-TESTING
APPLICATION OF PT/INR TESTING IN SCD
In the context of SCD, PT/INR testing serves multiple purposes, including monitoring anticoagulant therapy, assessing clotting status, and guiding treatment decisions. Anticoagulant therapy, such as warfarin, is commonly used in SCD patients to prevent thrombotic events, particularly in those with concomitant risk factors such as pulmonary hypertension or a history of stroke. PT/INR testing allows clinicians to titrate anticoagulant dosing to achieve the desired level of anticoagulation while minimizing the risk of bleeding complications.
PATIENT-CENTERED CARE
Involving SCD patients in research and treatment decisions is essential to ensuring that care is tailored to their individual needs and preferences. Patient engagement and advocacy play a crucial role in driving research agendas and promoting the development of innovative therapies and interventions for SCD.
THE BOTTOM LINE
Optimizing clotting control in SCD patients is essential for reducing the risk of thrombotic and bleeding complications and improving patient outcomes. PT/INR testing offers a valuable tool for clinicians to monitor coagulation status, tailor treatment approaches, and mitigate the risks associated with SCD-related coagulopathies. By integrating PT/INR testing into routine care protocols and advancing our understanding of SCD-related clotting issues, we can enhance the care and well-being of individuals living with this challenging condition.

Ensuring optimal PT/INR levels is crucial in the management of anticoagulant therapy, which often involves medications such as WARFARIN, commonly known as COUMADIN. Fortunately, the introduction of PT/INR monitoring devices has greatly simplified this process. These devices allow individuals to conveniently assess their PT/INR levels at home, providing prompt and accurate test results.